
For many seniors and their families, leaving a hospital or a skilled nursing rehab facility feels like crossing a finish line. The crisis has passed, the discharge papers are signed, and the comfort of home awaits.
Unfortunately, for a staggering number of older adults, this transition isn’t the end of a medical episode—it is the beginning of a revolving door.
Within days of returning home, a subtle shift occurs. A medication dose is missed because the new prescription looks different from the old one. A senior skips a meal because they are too fatigued to stand at the stove, leading to a sudden drop in blood sugar. A minor trip over a rug results in a devastating fall. Suddenly, the flashing lights of an ambulance are back in the driveway, and the senior is readmitted to the emergency room.
This is the “Rehab-to-ER” cycle—a frustrating, costly, and emotionally draining phenomenon that derails recovery, erodes independence, and accelerates cognitive and physical decline.
The good news? This cycle is highly preventable. By understanding the hidden risks of the post-discharge window and layering structured, professional caregiving into the home, families can break this cycle entirely. This comprehensive guide explores why the transition home fails so frequently and how dedicated caregiving transforms a vulnerable living space into a secure haven for long-term healing.
1. The Real Cost of the Revolving Door
Hospital readmissions are one of the most significant and complex challenges in modern geriatric healthcare. The statistics surrounding post-discharge complications highlight just how vulnerable seniors are during this critical window.
- The 30-Day Window: National healthcare data reveals that roughly 1 in 5 Medicare beneficiaries discharged from a hospital are readmitted within 30 days.
- The Cognitive Toll: For seniors managing existing cognitive vulnerabilities, such as Alzheimer’s disease or Parkinson’s disease, the physical stress of bouncing between a sterile hospital, a rehabilitation center, and home can induce transitional delirium—a state of acute confusion that significantly increases fall risks and functional decline.
- The Financial and Emotional Burden: Frequent emergency room visits drain retirement savings through co-pays and deductibles, exhaust primary family caregivers, and instill a deep sense of helplessness in the senior, who may begin to feel that regaining their independence is impossible.
2. Anatomy of a Relapse: Why the Transition Fails
To break the Rehab-to-ER cycle, we must first dissect exactly why the home environment becomes hazardous immediately following a discharge. It is rarely a single, catastrophic mistake; rather, it is a compounding series of minor operational breakdowns.
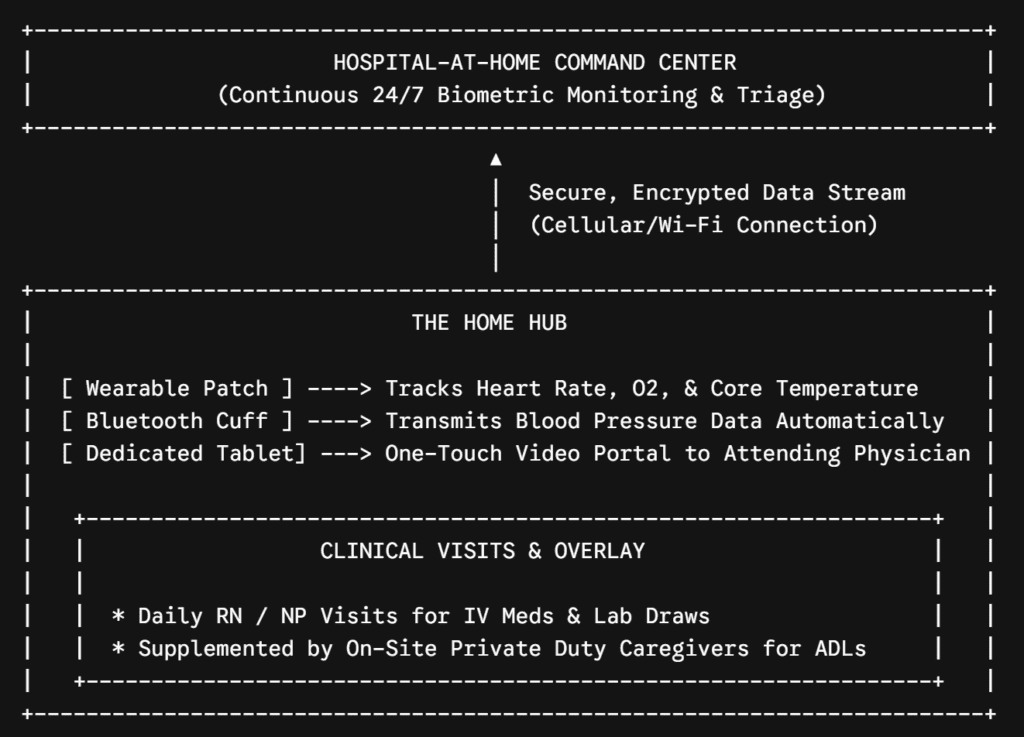
As shown in the framework above, a successful discharge fragments when three core pillars of health fail to transfer from the facility to the household:
A. Medication Mismanagement and Reconciliation Failures
In a hospital or inpatient rehab facility, medication administration is strictly controlled by electronic medical records, automated dispensing carts, and licensed nurses. The moment a senior steps across their own threshold, that entire clinical safety net vanishes.
A typical discharge introduces an average of three to five new medications—such as blood thinners, heavy-duty antibiotics, or modified dosages of heart medications. At the same time, the facility may instruct the patient to discontinue several of their old maintenance drugs.
Without a clinical background, an elderly individual or an overwhelmed family member is forced to sort through a confusing collection of pill bottles. The results can be disastrous: double-dosing on look-alike pills, skipping vital diuretics, or failing to complete a course of antibiotics, causing the underlying infection to return with a vengeance.
B. Physical Fatigue vs. The Illusion of Recovery
In the weeks spent recovering in a skilled nursing facility, seniors spend their days in a highly modified environment. The hallways have continuous handrails, the floors are perfectly flat commercial vinyl, the toilets are raised, and physical therapists are always within arm’s reach.
When seniors return home, they are often hit with a wave of psychological comfort that masks their actual physical limitations. They attempt to navigate narrow hallways, step over thick rugs, or reach into high kitchen cabinets. Because their muscles have suffered from deconditioning (muscle wasting due to prolonged bed rest), their balance shifts unexpectedly, leading to high-impact falls that land them straight back in the emergency room.
C. Nutritional Deficits and Dehydration
Healing requires an immense amount of metabolic energy. A body recovering from major surgery, a severe bout of pneumonia, or a cardiac event demands nutrient-dense meals and consistent hydration to rebuild tissue and maintain stable blood pressure.
However, a senior living alone or with an aging spouse rarely has the stamina to go grocery shopping, chop fresh ingredients, cook over a hot stove, and clean up the kitchen. Consequently, they resort to highly processed, high-sodium convenience foods—which can trigger immediate fluid retention and destabilize congestive heart failure—or they simply skip meals entirely, leading to weakness, orthostatic hypotension (dizzy spells when standing up), and dangerous dehydration.
3. How Caregiving Acts as a Clinical Shield
Professional, non-medical in-home caregiving bridges the dangerous gap between clinical discharge instructions and daily household execution. Caregivers do not replace doctors or home health nurses; rather, they serve as the on-site operational execution team that ensures medical plans are actually followed.
The 24-Hour Transition Protocol
The first 24 to 72 hours following a discharge are the most volatile. A professional caregiving strategy begins the moment the facility doors open:
- The Safe Transport and Settling In: A caregiver or care manager assists with the physical discharge process, ensures all personal belongings are collected, safely transports the senior home, and carefully settles them into bed or a supportive recliner.
- Immediate Pantry and Pharmacy Runs: While the senior rests, the care team picks up the newly modified prescriptions from the pharmacy and stocks the refrigerator with fresh, nutrient-rich foods that align with any new dietary restrictions (such as a low-sodium or diabetic-friendly diet).
- The Living Space Audit: The caregiver immediately scans the home for new hazards that may not have been an issue before the hospitalization—such as loose extension cords running to newly delivered medical equipment, clutter blocking pathing to the bathroom, or inadequate lighting for nighttime mobility.
4. The Six Core Pillars of Readmission Prevention
To permanently break the Rehab-to-ER cycle, an in-home caregiver implements a daily management structure focused on the six primary drivers of medical relapse.
Pillar 1: Rigorous Medication Reminders and Tracking
While non-medical caregivers cannot legally prescribe, pour, or physically administer medications from a bottle into a patient’s mouth, they play an indispensable role in compliance:
| Task Category | Caregiver Action | Preventative Benefit |
| Visual Logs | Cross-referencing daily intake against a master tracking sheet. | Prevents double-dosing or forgotten evening doses. |
| Prompting | Providing verbal and physical reminders at exact hourly intervals. | Ensures critical therapeutic drug levels remain stable in the bloodstream. |
| Symptom Matching | Watching for immediate side effects (dizziness, nausea) after a new pill. | Allows the family to alert the physician before a side effect causes a fall. |
Pillar 2: Vital Sign and Symptom Tracking (The Early Warning System)
Most readmissions occur because a chronic condition deteriorates silently until it becomes a full-blown emergency. Caregivers act as an early warning system by tracking subtle physical shifts every single day.
For a client managing Congestive Heart Failure (CHF), a caregiver assists with a daily morning weigh-in. A sudden weight gain of 2 to 3 pounds in 24 hours, or 5 pounds in a single week, is a classic clinical sign of fluid retention. By documenting this shift immediately, the caregiver enables the family to contact the cardiologist, who can adjust the senior’s oral medications over the phone—completely avoiding an emergency room visit for acute shortness of breath.
Pillar 3: Fall Mitigation and Transfer Assistance
A post-hospitalized senior is at an elevated risk for falls due to muscle weakness, cognitive fatigue, and medication side effects. Caregivers provide hands-on stability during the most hazardous moments of the day:
- The Bedroom-to-Bathroom Pathway: A significant percentage of senior falls occur during unassisted, hurried bathroom trips in the middle of the night. A caregiver staying overnight provides immediate, steadying assistance during these midnight transfers.
- Shower and Grooming Security: Bathrooms are inherently slick, hard, and dangerous. Caregivers manage safe transfers onto shower chairs, assist with bathing, and ensure the senior is completely dry before attempting to stand and dress.
- Assisting with Physical Therapy “Homework”: When a physical therapist leaves a home health session, they leave behind a list of daily exercises. A caregiver provides the physical presence and verbal encouragement needed to ensure the senior safely performs these movements, speeding up muscle rebuilding.
Pillar 4: Advanced Nutritional Security and Hydration
As established, a healing body requires premium fuel. Caregivers completely remove the physical burden of meal management from the senior:
- Customized Meal Prep: Preparing small, frequent, visually appealing meals that stimulate appetite, which is often suppressed by heavy post-hospital medications.
- Hydration Tracking: Keeping a designated water pitcher or tracking glass nearby and offering regular fluid prompts. This simple act drastically reduces the incidence of UTIs and dehydration-induced dizzy spells.
- Dietary Compliance: Ensuring strict adherence to mechanically altered diets (such as pureed or soft foods for patients recovering from a stroke or dysphagia) to prevent life-threatening aspiration pneumonia.
Pillar 5: Coordination of Follow-Up Medical Care
A successful discharge relies heavily on timely follow-up appointments with primary care physicians and specialists—typically within 7 to 14 days of returning home. Yet, arranging this logistics chain can be overwhelming for families.
Caregivers stabilize this process by managing the calendar, ensuring the senior is dressed and ready on time, assisting them into a wheelchair or vehicle, and providing reliable transportation to local medical offices. Furthermore, caregivers can take structured notes during the appointment, ensuring that any new modifications to the care plan are accurately brought back into the household.
Pillar 6: Cognitive Guardrails and Transitional Comfort
Hospital stays are profoundly disorienting for individuals living with dementia. The bright lights, constant monitor alarms, and rotating shifts of strangers often trigger a severe spike in behavioral symptoms.
When returning home, a professional caregiver re-establishes a predictable, calming routine. By maintaining a quiet environment, managing lighting to combat late-afternoon sundowning, and using proven behavioral techniques, they lower the senior’s stress hormones. This cognitive stabilization directly impacts physical recovery, keeping blood pressure down and preventing the agitation that frequently leads to dangerous pacing or unassisted wandering.
5. The Critical Post-Discharge Checklist for Families
If your loved one is currently preparing for a discharge from a local hospital or rehabilitation facility, use this actionable operational checklist to ensure no details slip through the cracks:
- [ ] Request a Completed Medication Reconciliation Sheet: Ensure the discharging physician clearly details exactly which pre-hospitalization medications should be restarted and which ones must be permanently thrown away.
- [ ] Secure a Minimum 14-Day Supply of New Prescriptions: Do not leave the facility without ensuring the new medications are either routed to a local pharmacy that delivers or are handed to you in physical form.
- [ ] Confirm Home Health Orders: Clarify if a Medicare-funded home health agency will be sending physical therapists or nurses, and establish exactly what days they plan to arrive.
- [ ] Schedule the Private Duty Caregiver Shift Overlay: Coordinate with your private duty caregiving team to ensure an aide is physically waiting at the house before the transport vehicle arrives, avoiding any unassisted gaps in care.
- [ ] Set Up Immediate Durable Medical Equipment (DME): Ensure that any required hospital beds, oxygen concentrators, walkers, or wheel-in commodes are completely installed inside the bedroom before the senior enters the front door.
Conclusion: Securing Lasting Recovery at Home
Breaking the Rehab-to-ER cycle requires moving away from reactive firefighting and embracing a proactive, structured framework of continuous home safety. The home shouldn’t be a place where seniors are left to navigate complex medical recoveries in isolation.
By introducing a professional caregiving structure during the incredibly vulnerable post-discharge window, you build an ironclad protective perimeter around your loved one. Caregivers seamlessly handle the physical, nutritional, and operational complexities of daily life, allowing your parent or spouse to focus entirely on what matters most: resting, regaining their strength, and permanently preserving their independence in the place they love most.
💡 High-Yield SEO Strategy for Implementation
To maximize the search authority and organic reach of this comprehensive article, structure its deployment using the following core SEO framework:
| Optimization Layer | Implementation Strategy | Target Value |
| Hyper-Local Inclusions | Weave in references to regional healthcare hubs (e.g., local San Diego institutions like UC San Diego Health, Sharp HealthCare, or Scripps Health) within the introductory or checklist sections. | Captures geo-targeted search phrases used by families looking for immediate local care solutions. |
| The “People Also Ask” FAQ Block | Embed 3 to 4 direct, single-sentence question headers (e.g., “Does Medicare pay for 24/7 care after a hospital stay?”) with immediate, clear text blocks below them. | Increases the probability of winning featured snippets and rich search result placements on Google. |
| High-Intent Lead Callouts | Place distinct, visually isolated contact blocks offering a “Post-Hospital Discharge Consultation” linking directly to your local care assessment forms. | Successfully converts high-stress informational readers into active, qualified care inquiries. |




