
Managing a progressive neurological condition like Parkinson’s disease (PD) at home requires a delicate balance of physical safety, strict clinical routines, and emotional support. Because Parkinson’s affects both the motor systems that control movement and the non-motor systems that govern mood, digestion, and sleep, home care must be holistic and adaptive.
This comprehensive guide offers evidence-based strategies, practical home modifications, and specialized care techniques designed to help family caregivers and home care professionals maintain safety, dignity, and independence for individuals living with Parkinson’s.
1. Understanding Parkinson’s Disease Progression
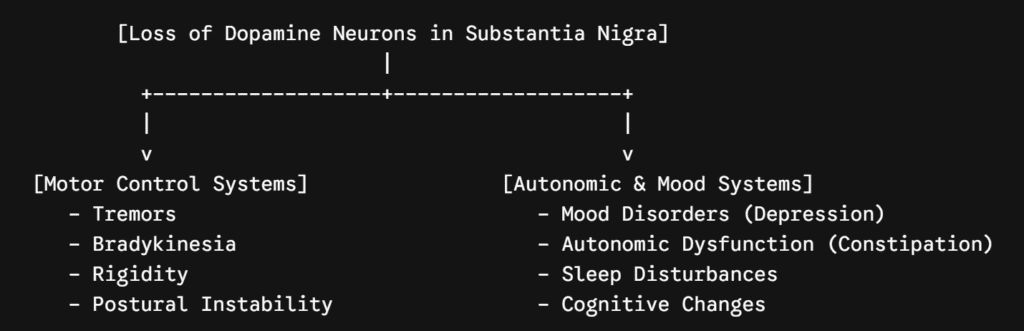
Effective home care begins with understanding that Parkinson’s is a highly individualized, progressive disorder. It is caused primarily by the loss of dopamine-producing neurons in a region of the brain called the substantia nigra. Dopamine is a chemical messenger critical for coordinating smooth muscle movements.
As dopamine levels drop, a person experiences characteristic motor adjustments. Simultaneously, the underlying neurodegenerative process often impacts other areas of the brain and the enteric nervous system (the “brain in the gut”), leading to a wide range of non-motor symptoms.
The Clinical Stages of Parkinson’s
Care needs shift significantly depending on the disease stage, typically classified using the Hoehn and Yahr scale:
- Early Stage (Stages 1–2): Unilateral or bilateral motor symptoms (e.g., a mild tremor in one hand, slight changes in posture or gait). The individual remains fully independent with activities of daily living (ADLs), though tasks may take longer.
- Mid Stage (Stage 3): Marked by the onset of postural instability (balance impairment). The individual experiences greater difficulty walking and turning, increasing the risk of falls. Independence with dressing, bathing, and eating is preserved but requires adaptive strategies or minimal supervision.
- Advanced Stage (Stages 4–5): Severe disability. Standing or walking without assistance becomes difficult or impossible; freezing episodes are frequent. Cognitive changes or Parkinson’s disease dementia (PDD) may emerge. The individual requires comprehensive, around-the-clock custodial care.
2. Managing Motor Symptoms at Home
The primary movement symptoms of Parkinson’s—tremors, bradykinesia (slowness of movement), rigidity (muscle stiffness), and postural instability—directly impact daily mobility and safety. Home care strategies must focus on preserving functional movement while minimizing the risk of injury.
Managing Freezing of Gait (FoG)
Freezing is a temporary, involuntary inability to move the feet, often described by individuals as feeling “glued to the floor.” It frequently occurs during environmental transitions, such as stepping through a doorway, turning around in a tight space, or moving from a carpeted room to a hard floor. Freezing is a primary driver of falls.
To manage freezing episodes at home, implement these behavioral and environmental strategies:
- Avoid Tight Turns: Instruct your loved one to make wide, looping turns (like a U-turn) rather than pivoting on one foot, which often triggers a freeze.
- Rhythmic Auditory Cues: Counting aloud (“1, 2, 3, step”), clapping a steady rhythm, or playing rhythmic marching music can help bypass the damaged basal ganglia and utilize the brain’s auditory pathways to initiate movement.
- Visual Cueing: Provide a clear visual target. Asking the individual to step over an object—such as a piece of brightly colored tape on the floor or the caregiver’s foot placed perpendicular to theirs—can break a freezing spell.
- Laser Walkers: For advanced stages, consider rollators or canes equipped with built-in laser modules that project a bright red line on the floor to serve as a continuous visual cue.
Promoting Safe Transfers and Mobility
Getting out of a bed, rising from a low chair, or transferring to a wheelchair require specific body mechanics to prevent strain on both the individual and the caregiver.
1.Prepare the Alignment:Before Moving.
Ensure the individual’s feet are flat on the floor, slightly apart, and positioned slightly behind the knees. This alignment creates a stable base of support and shifts the center of gravity forward.
2.Implement the Rocking Method:Initiating Momentum.
Instruct the individual to rock their upper body forward and backward three times while counting aloud. The phrase “Nose over toes” helps guide the chest forward over the knees to generate natural forward momentum.
3.Execute the Push-Off:The Stand.
Have the individual place their hands on the armrests of the chair or the edge of the firm mattress rather than reaching for the caregiver or a walker, which can tip over. Push upward using leg strength on the count of three.
4.Stabilize Before Walking:Post-Transfer Pause.
Once standing, instruct the individual to stand still for 5 to 10 seconds to ensure balance is secure and to allow any temporary blood pressure drops (orthostatic hypotension) to resolve before taking a step.
3. Creating a Safe, Parkinson’s-Friendly Living Environment
Physical modifications to the home are essential to counteract postural instability and prevent falls. Research shows that up to 60% of people with Parkinson’s experience a fall every year, making environmental remediation a high priority.
Living Room and Hallways
- Eliminate Tripping Hazards: Remove all throw rugs, loose mats, and electrical cords from walking pathways. Ensure transition thresholds between rooms are completely flat and secure.
- Furniture Selection: Replace soft, deep sofas and low coffee tables. Opt for tall, firm chairs with sturdy armrests and high seats. Avoid any chairs that swivel or are on wheels, as they can roll away unexpectedly during seating attempts.
- Clear Pathways: Maintain open walking lanes throughout the house that are at least 36 inches wide to accommodate walkers, rollators, or wheelchairs easily.
The Parkinson’s-Optimized Bedroom
Sleeping environments must balance comfort with ease of movement, as muscle rigidity can make rolling over or getting out of bed highly exhausting.
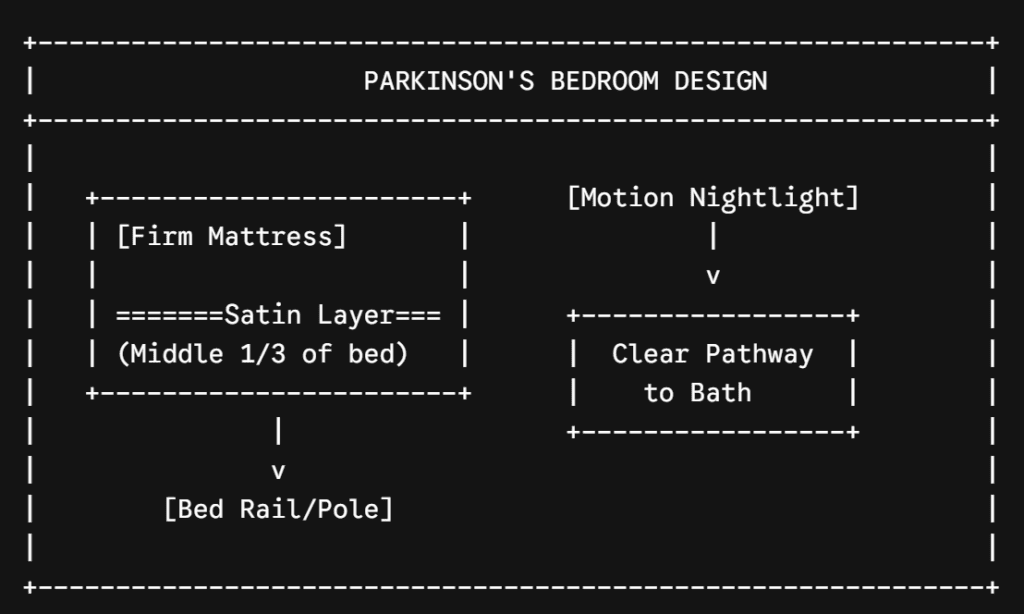
- Bedding Modifications: Place a section of slippery satin or silk fabric across the middle third of the bed (underneath the hips and shoulders). This reduces surface friction, making rolling over significantly easier. Avoid flannel sheets and heavy flannel nightwear, which create resistance against the mattress.
- Simplify Layers: Remove heavy top sheets and replace them with a single, lightweight down or alternative-fill comforter. This keeps the feet from becoming tangled or trapped during nighttime awakenings.
- Assistive Hardware: Install a heavy-duty bed rail or a floor-to-ceiling pressure-mounted bed pole next to the mattress. This provides a secure, immovable handgrip to assist with rolling and rising.
Bathroom Accessibility
The bathroom is a high-risk zone for slips and falls due to slick surfaces and confined spaces.
- Grab Bars: Install securely anchored grab bars near the toilet, inside the tub, and along the shower walls. Never rely on towel racks, glass doors, or soap dishes for weight support.
- Showering Adaptations: Place a slip-resistant rubber mat inside the tub or shower stall. Utilize a sturdy shower chair or a transfer bench with a backrest alongside a handheld showerhead to allow for safe, seated bathing.
- Toilet Alterations: Install an elevated toilet seat with integrated armrests or a surrounding toilet safety frame. Raising the seat height reduces the deep knee flexion required to sit, making standing back up much easier.
4. Addressing Non-Motor Symptoms: The Invisible Challenges
While motor symptoms are the most visible markers of Parkinson’s, non-motor symptoms often exert an equal or greater impact on an individual’s overall quality of life. These symptoms require proactive daily management.
Sleep Disturbances and Fatigue
Over 75% of individuals with Parkinson’s encounter sleep difficulties, including insomnia, sleep fragmentation, and REM Sleep Behavior Disorder (RBD), where patients physically act out vivid or violent dreams.
- Manage Daytime Sleepiness: Limit daytime napping to a single, scheduled 20-to-30-minute rest period in the early afternoon to protect nighttime sleep architecture.
- Evening Routine: Establish a predictable evening routine. Avoid caffeine, heavy meals, and screen exposure for at least two hours before bedtime.
- Safety Protocols for RBD: If the individual experiences severe dream-enactment behavior, ensure the immediate bedside area is clear of sharp corners, glass objects, or hard furniture to prevent injury from accidental falls out of bed.
Autonomic Dysfunction: Constipation and Low Blood Pressure
Parkinson’s slows down the smooth muscle contractions of the gastrointestinal tract, making severe constipation incredibly common. Additionally, many individuals experience Neurogenic Orthostatic Hypotension (nOH)—a sudden drop in blood pressure when changing positions.
- Dietary Fiber and Hydration: Aim for a high-fiber diet rich in whole grains, fruits, vegetables, and legumes. Ensure adequate hydration by encouraging fluids throughout the day (unless medically restricted), prioritizing water, herbal teas, or 100% fruit juices over caffeinated beverages.
- Combatting Blood Pressure Drops: To mitigate nOH, instruct the individual to transition slowly from lying to sitting, and from sitting to standing. Elevating the head of the bed by 10 to 15 degrees can also help regulate blood pressure dynamics overnight.
Mood Changes and Cognitive Health
Neurochemical shifts in the brain frequently induce clinical depression, anxiety, and apathy (a loss of motivation that is distinct from depression).
- Validate and Encourage: Apathy can look like a refusal to participate in care, but it is an organic symptom of dopamine depletion. Use gentle encouragement, keep choices simple, and maintain a predictable daily routine to reduce anxiety.
- Mental Stimulation: Keep the brain engaged through targeted cognitive exercises. Activities like puzzles, reading, strategy games, or music therapy help support cognitive flexibility and promote positive emotional health.
5. Medication Management and Timing Optimization
Pharmacological management—primarily via dopamine replacement therapy such as carbidopa/levodopa—remains the core approach for controlling Parkinson’s symptoms. However, these medications have a tight therapeutic window.
TYPICAL MEDICATION ADHERENCE PROFILE
Therapeutic Window (Smooth Movement) ==============
Delayed Dose (15-30 mins late) ------> "Off" Period: Tremors,
Rigidity, Immobility
The Crucial Importance of Timing
A delay in medication delivery of even 15 to 30 minutes can cause an individual to rapidly plunge into an “off” state, characterized by a return of severe rigidity, tremors, and a total loss of mobility.
- Strict Schedules: Use digital pill organizers with programmable acoustic alarms or smartphone applications to ensure medications are administered exactly at the prescribed intervals.
- Log Symptoms: Maintain a daily log tracking medication administration times alongside symptom fluctuations. Note when the medication takes effect (“on” times), when it begins to wear off, and any involuntary movements (dyskinesia) that may indicate a high dose. Bring this log to every appointment with the movement disorder specialist.
The Levodopa-Protein Interaction
Dietary protein can compete with levodopa for absorption across the intestinal wall and the blood-brain barrier, significantly reducing the medication’s effectiveness.
- Dosing Window: Administer carbidopa/levodopa at least 30 to 60 minutes before a protein-containing meal, or 2 hours after eating.
- The Carbohydrate Buffer: If the medication causes nausea when taken on an empty stomach, offer it alongside a small, non-protein carbohydrate snack, such as crackers, a piece of toast, or applesauce.
6. Nutritional Strategies and Swallowing Safety
As Parkinson’s progresses, the muscles involved in chewing and swallowing can weaken, leading to dysphagia (difficulty swallowing). This increases the risk of weight loss, dehydration, and aspiration pneumonia.
Safe Swallowing Protocols
- Upright Posture: Ensure the individual sits fully upright at a 90-degree angle during all meals and remains upright for at least 30 minutes after eating to prevent reflux and aspiration.
- The Chin-Tuck Technique: Instruct the individual to take a bite of food or a sip of liquid, hold it in their mouth, tuck their chin downward toward their chest, and then swallow. Tucking the chin physically alters the geometry of the pharynx, closing off the airway and opening the esophagus to ensure safe passage of food.
- Texture Modifications: Work alongside a speech-language pathologist (SLP) to modify food textures. Serve soft, moist, chopped, or pureed foods. If thin liquids trigger coughing spells, utilize commercial thickening agents to bring liquids to a nectar- or honey-like consistency.
High-Calorie, Nutrient-Dense Approaches
If tremors or slow eating lead to unintended weight loss:
- Frequent Small Meals: Transition from three large meals to five or six smaller, nutrient-dense meals throughout the day.
- Caloric Fortification: Add healthy fats like avocados, olive oil, smooth nut butters, and gravies to meals to boost caloric intake without increasing the total volume of food required.
7. Therapy, Exercise, and Rehabilitation at Home
Regular physical activity is a foundational, neuroprotective tool that preserves motor function, maintains joint flexibility, and counteracts muscle atrophy. All exercises should ideally be introduced under the guidance of physical or occupational therapists.
| Therapy Discipline | Focus Area for Parkinson’s Care | Primary Benefits |
| Physical Therapy (PT) | Gait training, balance exercises, core strengthening, and transfer safety. | Reduces fall risk, improves walking speed, and helps overcome freezing episodes. |
| Occupational Therapy (OT) | Fine motor coordination, adaptive tools, and home environmental safety assessments. | Enhances self-care independence (e.g., dressing, writing) and customizes home setups. |
| Speech-Language Therapy (SLP) | Vocal loudness (e.g., LSVT LOUD), articulation, and swallowing mechanism safety. | Combats a soft voice (hypophonia) and minimizes swallowing or choking hazards. |
Targeted Home Exercises
- Aerobic Activity: Encourage regular walking, stationary cycling, or water aerobics during “on” medication periods when mobility is at its peak.
- Mind-Body Practices: Tai Chi and yoga are excellent choices for individuals with Parkinson’s. These practices focus on weight-shifting, deliberate balance adjustments, and flexibility, which directly target postural instability.
- Fine Motor Upkeep: Activities like painting, clay modeling, or solving tactile puzzles help maintain manual dexterity and hand-eye coordination.
8. Preventing Caregiver Burnout: A Critical Component
Caring for a loved one with a progressive condition like Parkinson’s can be physically and emotionally demanding. Preventing caregiver burnout is vital for the long-term well-being of both the caregiver and the individual receiving care.
Practical Strategies for Family Caregivers
- Maintain Clear Boundaries: Avoid taking over tasks that your loved one is still capable of performing independently. Step-by-step assistance preserves their autonomy and reduces your daily physical workload.
- Utilize Respite Care Services: Schedule regular breaks by utilizing companion care services, adult day health programs, or short-term residential respite care. Taking time for your own physical health, social connections, and rest is essential.
- Join a Support Network: Connecting with specialized support networks, such as local chapters of the Parkinson’s Foundation or community caregiver support groups, provides valuable practical advice and emotional relief from peers who share similar experiences.
Summary Checklist for In-Home Parkinson’s Care
To ensure all aspects of care are covered, review this quick-reference home management checklist:
- [ ] Safety: Remove all throw rugs, widen pathways to 36 inches, and install bathroom grab bars.
- [ ] Bedroom: Install a bedside rail and place satin fabric across the middle third of the bed.
- [ ] Medication: Set up automated alarms to administer carbidopa/levodopa precisely on schedule.
- [ ] Nutrition: Time protein intake away from medication doses; implement the chin-tuck method if coughing occurs during meals.
- [ ] Exercise: Incorporate 20 to 30 minutes of daily movement (e.g., Tai Chi, walking) during “on” times.
- [ ] Support: Track symptoms in a daily log for medical appointments and arrange regular respite breaks for family caregivers.
