
When a parent or an aging spouse experiences a significant medical crisis—whether it is a severe flare-up of congestive heart failure, a complicated urinary tract infection (UTI) leading to delirium, or a slow recovery from major surgery—the immediate instinct for many families is panic.
Historically, a medical event of this scale meant an extended stay in an acute care hospital bed, followed by a stressful transition to a skilled nursing facility (SNF) or rehab center. Today, the landscape of healthcare is shifting rapidly. Advances in remote health technology, changing insurance models, and a overwhelming preference among seniors to age in place have birthed innovative care models designed to keep patients out of institutional settings entirely.
Two terms that families frequently encounter during these medical transitions are “Hospital-at-Home” care and “Traditional Private Duty Caregiving.”
While both models share the ultimate goal of supporting a senior in the comfort of their own residence, they serve entirely different structural, financial, and clinical purposes. Mistaking one for the other can lead to dangerous gaps in medical oversight or unexpected, heavy out-of-pocket financial bills.
This comprehensive guide breaks down the structural differences, clinical boundaries, financial realities, and exact scenarios where each service shines—giving you the exact blueprint needed to safeguard your loved one’s health and independence.
1. Defining the Core Models: What Are They?
To understand how these two systems interact, we must first look at them as two distinct pillars of home-based support: one is a temporary, highly clinical medical intervention, while the other is an ongoing, non-clinical supportive structure.
What is Hospital-at-Home Care?
Hospital-at-Home (HaH) is an innovative, acute-care model that delivers hospital-level medical services directly to a patient’s primary residence. Instead of lying in a standard, noisy inpatient hospital room, a patient who meets strict stability criteria is discharged to their own home, which is then rapidly transformed into a temporary clinical hub.
Under the Hospital-at-Home model, the patient remains technically admitted to the hospital system. They receive daily, face-to-face visits from registered nurses (RNs), regular examinations by physicians or nurse practitioners (often via advanced telehealth portals), and continuous biometric tracking. This model is acute, intensive, and strictly short-term—typically lasting only as long as a standard hospital stay (usually 3 to 5 days, up to a couple of weeks).
What is Traditional Private Duty Caregiving?
Traditional Private Duty Caregiving (often referred to as private duty home care, personal care, or non-medical home care) is a long-term, supportive service designed to help individuals with chronic illnesses, physical disabilities, or cognitive decline manage their Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs).
Private duty caregivers are professional aides (such as Certified Nursing Assistants or Home Health Aides) who provide hands-on assistance with tasks like bathing, dressing, grooming, mobility, meal preparation, medication reminders, and light housekeeping. This care is highly customizable, ranging from a few hours a week to comprehensive 24/7 live-in coverage. Unlike Hospital-at-Home, private duty caregiving is fundamentally non-clinical and is designed to sustain a person’s lifestyle and safety over months or years.
2. Head-to-Head Comparison: The Core Differences
When evaluating these options during a health crisis, it helps to compare their parameters side-by-side across critical categories such as medical authority, duration, and funding.
| Feature | Hospital-at-Home Care | Traditional Private Duty Caregiving |
| Primary Goal | Treat acute illness; replace an inpatient hospital stay. | Support daily functioning; manage chronic conditions long-term. |
| Clinical Level | High-level acute care (IV medications, oxygen, lab draws, diagnostics). | Non-clinical personal care (bathing, dressing, meals, companionship). |
| Medical Oversight | Attending physicians, hospitalists, and registered nurses (RNs). | Non-medical agency supervisors, family direction, or care managers. |
| Duration of Care | Short-term (typically 3 to 14 days total). | Long-term (ongoing for months, years, or indefinitely). |
| Technology Used | Continuous remote monitoring, dedicated cellular tablets, wearable sensors. | Simple logging apps, family communication portals, basic emergency pendants. |
| Primary Payer | Medicare, Medicare Advantage, and select private insurances. | Private pay out-of-pocket, Long-Term Care Insurance (LTCI). |
| Staffing Frequency | 1–2 nurse visits per day + 24/7 virtual on-call access. | Shift-based presence (e.g., 4 to 24 hours of continuous on-site care). |
3. Clinical Capabilities: Who Handles What?
The sharpest boundary line between these two services is the nature of the clinical tasks performed on-site. Understanding these boundaries is vital for patient safety.
The Clinical Power of Hospital-at-Home
Because Hospital-at-Home replaces an actual brick-and-mortar hospital room, it brings a suite of advanced diagnostic and therapeutic capabilities directly into the home environment. If a patient is admitted into an HaH program, the medical provider coordinates the rapid delivery of specialized medical equipment and clinical personnel.
- Advanced Diagnostics: Mobile imaging teams can arrive at the house to perform digital X-rays, ultrasounds, and electrocardiograms (EKGs) right at the bedside. Blood draws and point-of-care laboratory testing are completed daily to monitor electrolyte levels, kidney function, or inflammatory markers.
- Complex Therapies: Registered nurses administer continuous or intermittent intravenous (IV) medications, such as high-dose antibiotics for severe cellulitis or IV diuretics for acute congestive heart failure exacerbations. Advanced wound care, oxygen therapy management, and respiratory treatments are standard.
- Continuous Remote Monitoring: The home is outfitted with a continuous monitoring kit. Wearable patches or specialized devices automatically stream vital signs—heart rate, oxygen saturation, respiration rate, and blood pressure—directly to a centralized hospital command center staffed by clinical experts 24/7.
The Practical Support of Private Duty Caregiving
Private duty caregivers operate under strict state regulatory guidelines that prohibit them from performing invasive clinical or medical procedures. They are the eyes, ears, and hands of the household, focusing on the human, behavioral, and environmental factors that dictate a senior’s daily wellness.
- Hands-on Personal Care: Caregivers assist with critical physical transitions that present high fall risks. They help seniors safely transfer from bed to a wheelchair, navigate the bathroom, perform safe transfers during showers, and assist with incontinence care or toileting routines.
- Nutrition and Hydration Management: While a hospital dictates a clinical diet, a private duty caregiver actually stands in the kitchen to prepare the low-sodium meals required for a heart patient or the balanced, consistent meals needed for a diabetic. They provide consistent verbal encouragement to maintain hydration, which prevents a primary cause of geriatric hospital readmissions.
- Behavioral and Cognitive Support: For individuals dealing with cognitive impairments such as Alzheimer’s disease or Parkinson’s disease dementia, a caregiver provides orientation, structured daily routines, and gentle de-escalation during periods of late-afternoon confusion (sundowning).
The Care Gap Warning: A common point of confusion for families is assuming that a Hospital-at-Home program provides someone to sit with their parent all day to help them use the bathroom or cook meals. It does not. The hospital nurse arrives to perform clinical assessments and medical treatments, but then leaves. If your parent cannot safely stand up to cook or use the restroom independently between those nursing visits, they still require a private duty caregiver present in the home.
4. The Technology Shift: Transforming the Living Room by Hospital-at-Home
The explosion of the Hospital-at-Home model across the United States is primarily fueled by advancements in digital health technology. When a home is converted into an acute-care space, the technology deployed is sophisticated, industrial, and completely separate from consumer-grade smart devices.
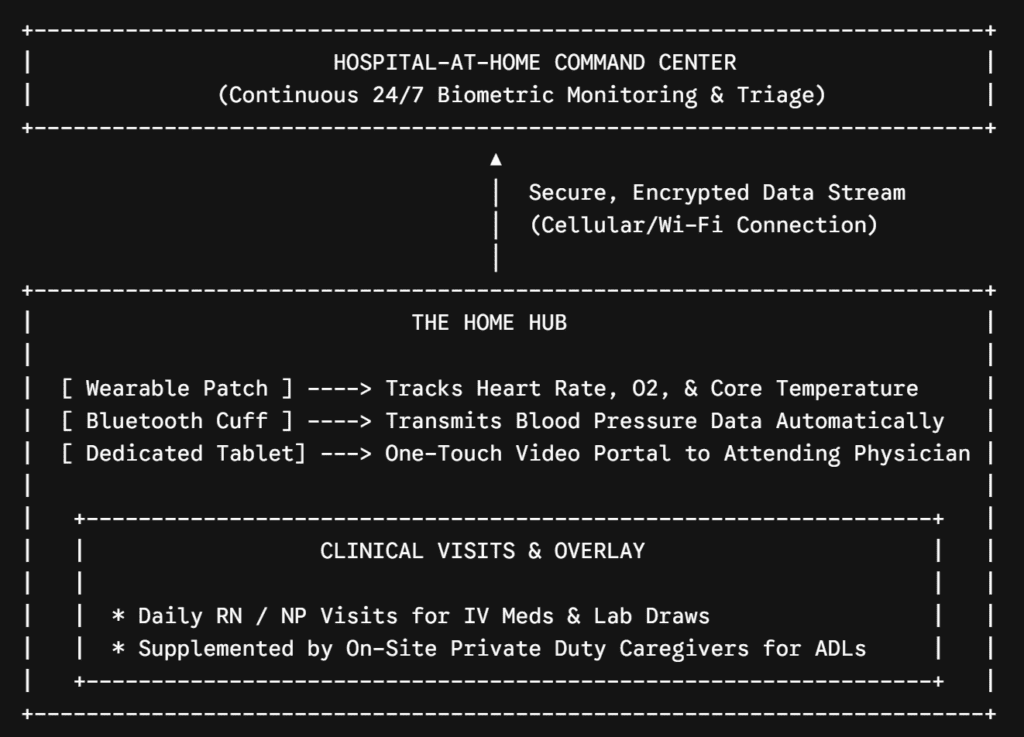
As illustrated above, the tech stack creates a continuous loop of clinical safety. The core components of this infrastructure include:
- The Central Communication Tablet: A dedicated, cellular-enabled tablet is set up by the hospital bed. It features a simplified, one-touch user interface allowing the patient or family caregiver to instantly launch a high-definition video call with the attending hospitalist or triage nurse at any hour of the night.
- Automated Biometric Peripherals: Bluetooth-enabled blood pressure cuffs, pulse oximeters, and weight scales automatically transmit data to the tablet the moment they are used. The patient does not need to write numbers down; the data streams instantly into the electronic health record (EHR) where algorithms watch for subtle deviations.
- Emergency Power and Backup Connectivity: Because a power outage or a dropped Wi-Fi signal could jeopardize patient safety, these systems are equipped with internal cellular backups and battery reserves, ensuring uninterrupted contact with the hospital command center.
Traditional private duty caregiving utilize a completely different, highly human tech footprint. Agencies typically deploy simple smartphone apps for caregivers to “clock in” using GPS verification, review a customized daily care plan checklist created by a supervisor, and log shift notes. These notes are designed to track baseline trends—such as sleep patterns, bowel movements, and mood fluctuations—rather than real-time clinical telemetry.
5. Financial Realities: Who Pays for the Care?
Navigating the financial architecture of senior care is often the most stressful hurdle for families. The payment mechanisms for Hospital-at-Home and private duty caregiving are entirely separate and rarely overlap.
Hospital-at-Home: Insurance and Medicare Coverage
Because Hospital-at-Home programs are certified acute-care extensions of major health systems, they are billed as regular inpatient hospital stays.
- The Medicare CMS Waiver: In late 2020, the Centers for Medicare & Medicaid Services (CMS) launched the Acute Hospital Care at Home program. Under this waiver, traditional Medicare covers 100% of the approved Hospital-at-Home costs for eligible patients, matching the exact payment structure of a traditional physical hospital stay. The patient is only responsible for their standard hospital deductibles and co-insurance.
- Commercial and Medicare Advantage Plans: Many major commercial health insurers and Medicare Advantage plans now explicitly cover HaH programs. There are zero out-of-pocket costs for the delivery of medical equipment, technological setups, or daily nursing visits beyond standard inpatient cost-sharing.
Private Duty Caregiving: The Private Pay Landscape
Traditional private duty caregiving is fundamentally categorized as a long-term, “non-medical” service. Because it does not require continuous skilled nursing licenses for standard daily shifts, public insurance options do not cover standard long-term maintenance care.
- Medicare Limitation: Traditional Medicare does not pay for private duty caregiving if the senior only requires assistance with daily tasks like bathing, dressing, or meal preparation. While Medicare has a benefit called “Home Health Care,” this is strictly limited to short-term, intermittent visits from physical therapists or skilled nurses following an acute event, lasting only a few hours per week. It does not provide shift-based coverage.
- Private Pay (Out-of-Pocket): The vast majority of families fund private duty caregiving out-of-pocket using personal savings, retirement income, investment portfolios, or the proceeds from liquidating real estate assets.
- Long-Term Care Insurance (LTCI): If your loved one purchased a private long-term care insurance policy years ago, these policies are explicitly designed to fund private duty personal care. To trigger the policy benefits, the senior must typically demonstrate a deficiency in a set number of Activities of Daily Living (usually 2 out of 6, such as bathing and transferring) or have a diagnosis of cognitive impairment requiring continuous supervision.
6. How the Two Models Coexist: A Real-World Scenario
To fully appreciate the synergy between these two models, let us look at a common real-world scenario that plays out in families across the country every single day.
The Case of Margaret: Chronic Illness Exacerbation
Margaret is an 82-year-old grandmother living at home. She manages moderate-stage Alzheimer’s disease and chronic obstructive pulmonary disease (COPD). Her daughter, Sarah, works a demanding full-time corporate job and manages her mother’s care from a distance.
One Tuesday morning, Margaret develops a severe respiratory infection, causing her oxygen levels to drop and triggering a massive spike in confusion and agitation due to her underlying dementia.
Here is how the two care models deploy simultaneously to handle the crisis smoothly:
[ Tuesday Morning: Crisis Occurs ]
│
▼
[ Hospital-at-Home Deploys ] ───► * Installs remote oxygen monitoring
│ * Initiates IV antibiotic therapy
│ * Doctor conducts virtual daily rounds
▼
[ The Care Gap Identified ] ───► Margaret is too confused to manage meals,
│ use the bathroom safely, or stay calm
│ between short nurse visits.
▼
[ Private Duty Aides Step In ] ─► * Provides 12-hour on-site presence
* Prepares soft meals & manages fluid intake
* Keeps Margaret calm during "Sundowning"
* Safely transfers her to prevent falls
By layering these two models, Margaret gets the intensive clinical intervention required to cure her acute respiratory infection without the terrifying disorientation of a sterile hospital room, while her daily human needs are met continuously by a dedicated personal aide. Sarah can rest assured that her mother is medically secure and physically protected without having to take an extended, unpaid leave of absence from her career.
7. Choosing the Right Path between Hospital-at-Home’ Care vs. Traditional Private Duty Caregiving
If you are currently standing in a hospital hallway or sitting at a kitchen table trying to determine the next best step for an aging parent, utilize this simple decision framework to guide your family’s strategy.
Choose Hospital-at-Home Care If:
- The condition is acute but stable: The patient has a specific, treatable medical diagnosis (like pneumonia, cellulitis, dehydration, or a mild heart failure flare) that requires hospital-level treatments like IV fluids or continuous monitoring, but they do not require an Intensive Care Unit (ICU) or immediate surgical access.
- Hospital delirium is a primary risk: The senior suffers from cognitive decline or dementia. Taking them out of their familiar environment will trigger severe confusion, behavioral outbursts, or a rapid loss of functional baseline metrics.
- An eligible health system is managing care: The patient’s primary medical provider or local hospital group operates an approved, integrated Hospital-at-Home program covered by their insurance.
Choose Traditional Private Duty Caregiving If:
- The primary challenges are functional, not medical: The senior is medically stable but can no longer safely navigate their home independently, struggle to cook balanced meals, forget to take their daily maintenance medications, or require physical assistance with showering and toileting.
- Long-term preservation of independence is the goal: The care needs are chronic and ongoing. There is no expectation that the need for assistance will disappear in two weeks; rather, the family is setting up a stable, long-term care infrastructure to support aging in place.
- Respite for family caregivers is desperately needed: The primary family caregiver is experiencing physical fatigue, severe mental stress, or professional disruption due to the constant demands of managing their parent’s home life.
Conclusion: Crafting a Balanced Care Ecosystem
The modern evolution of eldercare is moving away from the rigid, institutional pipelines of the past. No longer must a medical setback automatically mean a permanent relocation to a clinical facility.
By understanding that Hospital-at-Home care acts as an acute, high-powered medical umbrella during a crisis, while Traditional Private Duty Caregiving serves as the rock-solid, daily human foundation of safety, families can design a highly coordinated care ecosystem.
When applied strategically, these services do not compete—they connect. They give adult children the ultimate peace of mind: knowing that their aging parents are receiving top-tier medical care and compassionate personal support, right where they want to be most: at home.




